Assessing the Knowledge, Practices and Attitude of Pharmacists, Prescribers and the Community Toward Antimicrobial Resistance in Ghana
-
Osisiogu Udochukwu Emmanuel

Department of Science Laboratory Technology, Dr. Hilla Limann Technical University, Wa, Ghana
Fahad Bin WaqasDepartment of Medical Laboratory Technology, Faculty of Allied Health Sciences, Radford University College, Lagos Ave, Accra, Ghana
Calebina Ayeyi AppiahDepartment of Physician Assistantship, Faculty of Allied Health Sciences, Radford University College, Lagos Ave, Accra, Ghana
Fareeda Ceeta MahmoudDepartment of Physician Assistantship, Faculty of Allied Health Sciences, Radford University College, Lagos Ave, Accra, Ghana
Emmanuel Mawuli NattahDepartment of Molecular, Claron Health International, Accra, Ghana
Regina Ama BanuCouncil for Scientific and Industrial Research, Water Research Institute, Accra, Ghana
Amanda Eyram BaniniDepartment of Accounting and Finance, Kwame Nkrumah University of Science and Technology, Kumasi, Ghana
| Received 18 Feb, 2023 |
Accepted 15 Jun, 2023 |
Published 25 Jul, 2023 |
Background and Objective: Antimicrobial Resistance (AMR) is a burgeoning threat to the interests of public health globally. Significant data indicates that the management of AMR depends on the information and attitudes of the community, as well as those of pharmacists and doctors, therefore this study sought to investigate the knowledge base of the aforementioned groups on AMR. Materials and Methods: Purposive sampling technique was used to gather data from this cross-sectional survey that included 766 participants and three different self-administered questionnaires were given to the randomly selected sample population of 652, 51 and 63 community members, clinicians and pharmacists, respectively. Results: There was a significant association between educational level and whether individuals who consumed antibiotics without a doctor’s prescription reportedly insisted on an antibiotic prescription. Almost half of the respondents acknowledged that they often dispose of antibiotics alongside household waste. The majority of the physicians in this study knew about the nonclinical/environmental routes for the spread of AMR genes and the physicians felt AMR was a problem they encountered daily. Conclusion: This study has identified potential avenues aimed at designing tri-faceted interventions for controlling the development and dissemination of AMR.
| Copyright © 2023 Emmanuel et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
Antimicrobials are one of the most successful forms of chemotherapy in the history of modern medicine1. They have played an undeniable role in reducing morbidity and mortality attributable to infectious diseases since their introduction in the 1940s2. However, the development and subsequent dissemination of Antimicrobial Resistance (AMR) pose a universal threat to humans, animals and the environment3.
AMR is a phenomenon that can occur naturally and its perpetuation has been considerably worsened by the inappropriate use of antibiotics. Over the last decades, bacteria responsible for both common and severe life-threatening infections have consistently acquired resistance to novel antibiotics. AMR has become an issue of global relevance. Reports from Low and Middle-Income Countries (LMICs) indicate an exponential increase in the rates of AMR, including the dissemination of novel multidrug-resistant strains of medically important microbes4-6. Common diseases with bacteriologic etiology such as Respiratory Tract Infections (RTIs), Some Sexually Transmitted Infections (STIs) and Urinary Tract Infections (UTIs), are rapidly becoming untreatable. Life-saving medically invasive procedures are becoming riskier and food systems are becoming increasingly insecure7. By 2030, AMR could force up to 24 million people into extreme poverty and result in up to 10 million deaths each year by 20508. However, this projection requires scrutiny from population-based surveillance network datasets that factor in morbidity and mortality figures, especially from Low to Middle-Income Countries (LMICs). Until such data is made available, global AMR burden estimates are not entirely reliable and will not be able to inform meaningful action9. Nonetheless, incertitude about forecasting morbidity and mortality does not take away from the overall seriousness of AMR9.
World Health Organization (WHO) declared AMR a phenomenon of high priority to be resolved by a collective global action. The plan outlines five objectives that point to a “One Health” scheme that incorporates directives for human, veterinary medicine, food and the environment10. Initiatives such as the introduction of the Global Antimicrobial Resistance Surveillance System (GLASS) in 2015 by the WHO have ushered burgeoning awareness among many countries around the globe to forestall AMR11.
Despite these global efforts, AMR is having an unprecedented effect on the ability of medical practitioners to control the increasing range of infections caused by resistant microbes12. Such observations are a result of a multifactorial interplay between inadequate patient education on antimicrobials in general, a substandard diagnostic approach due to lack of knowledge, personnel and or infrastructure, improper prescription practices amongst clinicians, unauthorized and or unwarranted sale of antimicrobial agents by pharmacists and non-human consumption of antimicrobials due to agricultural practices.
This radical interplay might significantly vary depending on the geographies of both developing and developed nations. Therefore, intercessory efforts would require that measures be specific to the locale in question13. The negative effects of AMR are seemingly unpreventable but can be considerably curbed and therefore must be controlled through approaches that are both multifaceted and multidisciplinary4.
AMR is fast emerging as an issue of concern in Ghana and bears significant public health repercussions14. This is evidenced by the marked increase in the isolation of antimicrobial-resistant organisms from patient specimens across the country15. Numerous local studies have revealed the alarming prevalence of resistant microbes to commonly prescribed and utilized antibiotics such as ampicillin, chloramphenicol, cotrimoxazole and tetracycline16,17. A 2015 metareview of some Low and Middle-income Countries (LMICs) demonstrated that the overall prevalence of antimicrobial self-medication was as high as 38.8%18. Another study reported levels of antibiotics (penicillin, amoxicillin and metronidazole) present in soil samples from landfills as high due to improper disposal practices and waste management19. Such findings only reinforce and corroborate the far-reaching and debilitating effects of AMR. It has been conclusively proven that an increase in oral antimicrobial therapy correlates with an increase in resistance, these findings are probably the result of poor prescription and dispensing practices for antibiotics, a lack of adherence to treatment plans and the use of cheap medications2. The inability to detect trends of resistance to widespread antibiotics in Ghana is significantly impacted by the lack of a national surveillance mechanism for monitoring AMR. In Ghana, the Over-The-Counter (OTC) availability of antibiotics and their subsequent abuse makes the problem a tri-faceted one involving clinicians, pharmacists and patients. There have not been any local studies that collectively assess the patient, physician and pharmacist knowledge-base and attitudes toward antibacterial chemotherapy in Ghana. Thus, it becomes necessary to evaluate the knowledge and gauge the practices of the aforementioned primary stakeholders in the battle against AMR.
MATERIALS AND METHODS
Study design and sampling technique: This study adhered to a cross-sectional design and depended on triple questionnaires administered to physicians, pharmacists and the general public on a randomly selected sample population. It relied on a purposive sampling technique (non-probability method) for data collection. The questionnaires were prepared in concordance with the expected professional knowledge base of the respective groups for which it was intended. The survey was conducted between May and July, 2020 by the declaration of Helsinki20.
Study site: This study was conducted in Ghana, a country located in West Africa and sandwiched between Cote d'Ivoire (Ivory Coast) and Togo. The northern border is the country Burkina Faso and the southern border is the Gulf of Guinea. The majority of the respondents originated from the Greater Accra and Upper West Regions, with a few distributed between regions such as Western Region, Ashanti Region and Bono East Region, respectively. The country has a general population of approximately 30 million people as of May, 202021.
Sample size: A total of 766 individuals participated in this study, 51 clinicians, 63 pharmacists and 652 members of the general public.
Reliability and scoring: The internal consistency of the questions was analyzed employing Cronbach’s α test22. The results of the three different data sets were found to be reliable (i.e., 0.70, 0.73 and 0.71 for the community, pharmacists and physicians, respectively). To enhance the coherence of the datasets, “strongly agree” or “agree” were classified as agreed and “strongly disagree” or “disagree” as disagreed.
Statistical analysis: The data were analyzed using SPSS (version 23.0) set at a 95% confidence interval (p-value<0.05) statistically significant. The results were summarized by highlighting the percentage distribution in different categories. Key associations between demographic information and responses were analyzed via the Chi-square Test of association, Fisher’s exact test and Mann Whitney U-Test. The choice of statistical tests was dependent on factors such as the response scale and whether or not the distributions met the peculiar statistical assumptions of the tests involved.
RESULTS
Results for public: A total of 652 responses were received from the public residing in 14 of the 16 Regions of Ghana. Of the distribution, 414 (63.5%) were male while 237 (36.3%) were female. The 565 (86.7%) individuals were below 30 years of age, while 87 (13.3%) were in the 31-60 age bracket. The majority of the responses were from the Greater Accra Region (47.5%) and Upper West Region (46.6%). The remaining 5.9% of the distribution was from 12 other regions with no response received from the Ahafo and Upper East Regions. Generally, respondents in urban areas (77.5%) outnumbered those dwelling in rural areas (22.5%). The 568 (87.1%) had tertiary education, 81 (12.4%) had a high school education and only 3 (0.5%) had no formal education. The professional backgrounds of the respondents varied, with students comprising the majority of the distribution (62.6%), followed by individuals who identified with the “other” group (16%). Government employees and entrepreneurs made up 12.4 and 8% of the total population, respectively. To grasp basic information on antimicrobial resistance to the public, some general questions were asked (Table 1).
| Table 1: | General questions to the public | |||
| Question | Agree |
Disagree |
Do not know |
| AMR is the tolerance level of the body after which the | 362 (55.5%) |
133 (20.4%) |
157 (24.1%) |
| body gets used to the antibiotic | |||
| AMR is a global problem | 412 (63.2%) |
72 (11.0%) |
168 (25.8%) |
| Common cold can be cured with a course of antibiotics | 346 (53.1%) |
214 (32.8%) |
88 (13.5%) |
| AMR organisms can cause death | 384 (58.9%) |
71 (10.9%) |
197 (30.2%) |
| Table 2: | General questions to the public | |||
| Question | Yes |
No |
| I have consumed antibiotics without a doctor’s prescription before | 437 (67.0%) |
215 (33.0%) |
| I feel I know when to use antibiotics for common problems | 282 (43.3%) |
370 (56.7%) |
| I have insisted on an antibiotic prescription from the doctor before | 207 (31.7%) |
445 (68.3%) |
| I always complete the course of treatment with antibiotics even if I feel better | 356 (54.6%) |
296 (45.4%) |
| before the completion | ||
| I prefer to keep antibiotics at home in case there may be a need for them later | 425 (65.3%) |
226 (34.7%) |
| It is okay to get antibiotics from relatives or friends without having to see a medical doctor | 95 (14.6%) |
557 (85.4%) |
| I prefer to be able to buy antibiotics from the pharmacy without a prescription | 212 (32.5%) |
439 (67.5%) |
| I prefer to use an antibiotic if I have a cough for more than a week | 266 (40.8%) |
386 (59.2%) |
| When I have a sore throat I prefer to use an antibiotic | 296 (45.5%) |
355 (54.5%) |
| I often dispose of my antibiotics along with the household waste | 318 (48.8%) |
334 (51.2%) |
The 31.7% (n = 207) of individuals agreed that they have insisted on an antibiotic prescription (Table 2). However, there was no significant association between this practice and gender, occupation, educational background, or area of settlement (rural or urban). The 48.4% (n = 318) of respondents acknowledged that they often dispose-off antibiotics alongside household waste (Table 2). Neither educational background nor the area of settlement had any significant association with this finding. However, there was a statistically significant association between gender and this practice (X2 (2) = 10.77, p = 0.002). The 65.3% (n = 425) of individuals claimed that they stored antibiotics at home to fulfill a later need and 45.4% (n = 296) admitted to not completing an antibiotic course (Table 2).
Fisher’s exact test revealed no association between gender and whether individuals consumed antibiotics without a doctor’s prescription. However, there was a statistically significant association between educational level and this practice (X2 (2) = 17.89, p = 0.00). The effect size for this finding, Cramer’s V, was weak, 0.17 (X2 is the Chi-square statistic and Cramer’s V describes effect size).
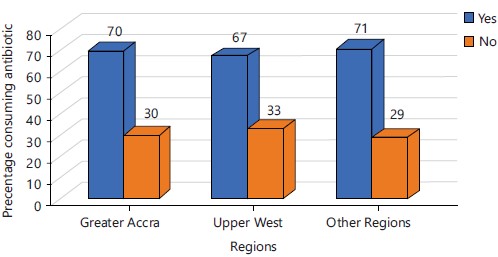
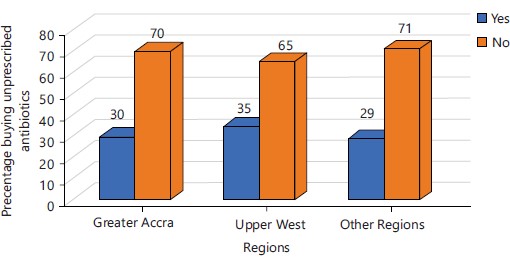
Figure 1 demonstrated an approximate equality between individuals consuming antibiotics without a prescription across regions while, Fig. 2 demonstrated a majority trend of individuals answering “No” to having bought antibiotics without a prescription. The interplay between these two groups of responses reveals a discrepancy suggestive of weak dispensation practices at pharmacies.
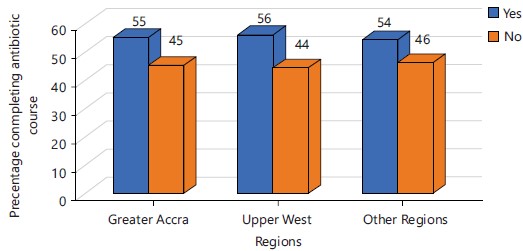
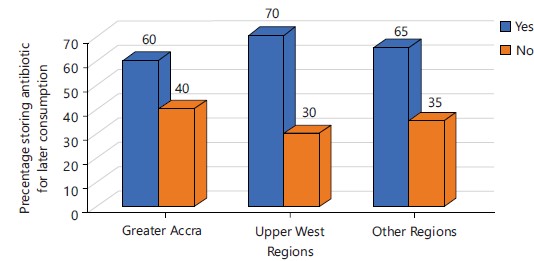
There was a discernable trend in responses across regions when individuals were queried about the completion of antibiotic regimens. However, approximately 50% of participants did not complete their course of antibiotics (Fig. 3). On the other hand, a similar negative trend was observed for individuals who stored antibiotics with the intent of later consumption on a need-basis (Fig. 4).
Results for clinicians: A total of 51 clinicians participated in this category comprising 56.9% (n = 29) and 43.1% (n = 22) males and females respectively. 45% of clinicians were based in the Greater Accra Region with 96.1% (49) of all clinicians being between 21-40 years of age and 76% (n = 39) of them possessing a considerable working experience of between 1-5 years. The 72.5% (37) of clinicians confirmed that patients made demands for antibiotics to treat conditions such as the common cold thus 74.5% (38) of the clinicians considered AMR as a serious problem in their daily clinical practice (Table 3). They further corroborated this when 82.4% (42) of them agreed that ABR infections could further complicate medical procedures like surgery, organ transplants and cancer treatments. The 70.6% (36) clinicians claimed to have received some teaching/training on antibiotic resistance spread (Table 3).
|
|
| Table 3: | General questions for clinicians | |||
| Question | Agree |
Disagree |
Do not know |
| Do patients demand an antibiotic treatment for a common cold? | 37 (72.5%) |
14 (27.5%) |
Not applicable |
| Do you think antibiotic-resistant infections could make medical procedures like surgery, organ transplants and cancer treatment much more? Dangerous? |
42 (82.4%) |
9 (17.6%) |
Not applicable |
| Antimicrobial resistance is a problem in my daily practice | 38 (74.5%) |
11 (21.6%) |
2(3.9%) |
| Development of a local guideline would be more useful than the international ones for antimicrobial resistance |
39 (76.5%) |
9 (17.6%) |
3 (5.9%) |
| Antibiotic guidelines and antibiotic committees are an obstacle more than a help to clinical care |
10 (19.6%) |
33 (64.7%) |
8 (15.7%) |
| I feel there is a need to organize educational/ awareness programs on antibiotic resistance in the community |
50 (98.0%) |
1 (2.0%) |
Not applicable |
| Patient demands antibiotics contribute to over-prescriptions and overuse | 42 (82.4%) |
8 (15.7%) |
1 (1.9%) |
| During the last 5 years, I have received some teaching/training on antibiotic resistance spread |
36 (70.6%) |
15 (29.4%) |
Not applicable |
| I know about the nonclinical/environmental routes for the spread of antimicrobial resistance genes |
38 (74.5%) |
8 (15.7%) |
5 (9.8%) |
Cross tabulation via Fisher’s Exact Test showed that neither gender nor work experience had any statistical bearing on the results for AMR being a daily problem in clinical practice. There was no significant association between clinician gender or work experience and whether they agreed that ABR infections could further complicate medical procedures.
Results for pharmacist: A total of 63 responses were received from pharmacists comprising 52 males (82.5%) and 11 females (17.5%). The 61 (96.8%) were between the ages of 21 and 40. The majority (60.3%) had between 1-4 years of working experience. The 96.8% (n = 61) pharmacists agreed that antimicrobial surveillance programs would improve patient care while 92.1% agreed that adequate training should be provided to community pharmacists on antimicrobial use (Table 4). This demonstrated an obvious will within pharmacists to partake in educational programs to reduce AMR.
|
|
| Table 4: | General questions for pharmacists | |||
| Question | Agree |
Disagree |
Do not know |
| AMS programs improve patient care | 61 (96.8%) |
2 (3.2%) |
Not applicable |
| AMS should be incorporated at the community pharmacy level | 58 (92.1%) |
4 (6.3%) |
1 (1.6%) |
| AMS programs reduce the problem of antimicrobial resistance | 56 (88.9%) |
5 (7.9%) |
2 (3.2%) |
| Adequate training should be provided to community pharmacists on antimicrobial use |
61 (96.8%) |
1 (1.6%) |
1 (1.6%) |
| Relevant workshops and other educational activities are required to be attended by community pharmacists to enhance their understanding of AMS |
58 (92.1%) |
2 (3.2%) |
3 (4.8%) |
| Individual efforts at AMS have minimal impact on the issue of antimicrobial resistance |
33 (52.4%) |
27 (42.8%) |
3 (4.8%) |
| I think that the prescribing physicians are the only professionals who need to understand AMS |
9 (14.3%) |
53 (84.1%) |
1 (1.6%) |
| Pharmacists have a responsibility to take a prominent role in AMS and infection control programs in the health system |
60 (95.2%) |
1 (1.6%) |
2 (3.2%) |
The 19% of pharmacists reported that they only “occasionally” dispensed antimicrobials after having obtained complete clinical information, while 9% admitted to dispensing antimicrobials without ever obtaining clinical information (Table 5).
| Table 5: | Questions about the practice of pharmacists | |||
| Question | Never |
Rarely |
Occasionally |
Often |
Always |
| I dispense antimicrobials on prescription having | 9 (14.3%) |
2 (3.2%) |
12 (19.1%) |
20 (31.7%) |
20 (31.7%) |
| obtained complete clinical information | |||||
| I dispense antimicrobials without a prescription | 15 (23.8%) |
17(27%) |
22 (34.9%) |
8 (12.7%) |
1 (1.6%) |
| I sometimes dispense antimicrobials for durations more than prescribed by the physician on the patient’s applicable |
50 (79.4%) |
5 (7.9%) |
7 (11.1%) |
1 (1.6%) |
Not request |
| I sometimes dispense antimicrobials for durations more than prescribed by the physician based on my discretion |
29 (46%) |
12 (22.2%) |
17 (27.0%) |
3 (4.8%) |
Not applicable |
| I screen the antimicrobial prescription by local guidelines before dispensing |
3 (4.8%) |
5 (7.9%) |
9 (14.3%) |
16 (25.4%) |
30 (47.6%) |
| I collaborate with other health professionals for infection control and antimicrobial stewardship |
3 (4.8%) |
12 (19%) |
11 (17.5%) |
24 (38.1%) |
13 (20.6%) |
| I communicate with prescribers if I am unsure about the appropriateness of an antibiotic prescription |
Not applicable |
Not applicable |
7 (11.1%) |
18 (28.6%) |
38 (60.3%) |
| I seek additional clinical information (e.g. drug interactions, adverse drug reactions, allergy, etc.) before deciding to dispense the antibiotic prescribed |
Not applicable |
5 (7.9%) |
6 (9.5%) |
19 (30.2%) |
33 (52.4%) |
| I take part in antimicrobial awareness campaigns to promote the optimal use of antimicrobials |
5 (7.9%) |
9 (14.3%) |
20 (31.7%) |
14 (22.2%) |
14 (22.2%) |
| I educate patients on the use of antimicrobials and resistance-related issues |
Not applicable |
2 (3.2%) |
8 (12.7%) |
15 (23.8%) |
38 (60.3%) |
| I make efforts to prevent or reduce the transmission of infections within the community |
2 (3.2%) |
5 (7.9%) |
13 (20.6%) |
25 (39.7%) |
18 (28.6%) |
An independent two-sample t-test was conducted on a group of questions. Regarding dispensation of antimicrobials beyond durations prescribed by physicians based on personal experience, male respondents (M: 4.154, SD:0.9779) were not significantly different (t61 = 1.052, p>0.05) from female respondents (M: 3.818, SD: 0.8739) with a mean difference of 0.3357. This implied that neither gender was more likely to dispense prolonged doses of antibiotics based solely on personal experience.
Regarding the dispensation of antimicrobials beyond durations prescribed by physicians based on patient request, male respondents (M: 4.673, SD: 0.7335) were not significantly different (t61 = 0.514, p>0.05) from female respondents (M: 4.545, SD: 0.8202). This implied that neither gender was more likely to dispense prolonged doses of antibiotics based solely on patient request.
DISCUSSION
This is possibly the first comprehensive study conducted concurrently on the knowledge, attitudes and role of three main players in the context of AMR in Ghana. In Ghana, there are primary data on the use of antibiotics and the emergence of resistance. The most likely cause of this scarcity is a lack of money from the local administration and other NGOs. Antibiotic abuse and overprescribing have a long history in Ghanaian hospitals23. Concerns of antibiotic abuse are cause for a global quagmire, with individuals partaking in harmful practices such as storing antibiotics at home or utilizing them for the common cold. A study in Iraq indicated that 37.2% and 42.2% of participants respectively partook in the aforementioned practices24. However, the findings of this study showed that 65.2% prefer to store antibiotics at home for later use (Table 2).
A competing study in the Asian Sub-Continent reported that 56.6% of respondents believed that antibiotics could cure all types of infections25. This finding was echoed in this study, with 43.3% of individuals believing they could self-medicate antibiotics for common problems and 45.4% of respondents thinking it was appropriate to use antibiotics for sore throats and some others believing it was okay to obtain antibiotics to treat a cough that lasted over a week (Table 2). A study in the UAE demonstrated that 3.65% of individuals obtained antibiotics from friends or family26 and this is similar to the findings of this current study. Abujheisha et al.26 also showed that 33.5 and 57% of individuals did not complete their prescribed course of antibiotics (on account of feeling better) and stored antibiotics for later consumption, respectively. The findings of this study were parallel to this since 45.4 and 65.2% did not complete prescribed courses and stored antibiotics for later use, respectively.
There seems to be an obvious semblance between public responses across Africa and Asia. This may be attributable to all countries involved being LMIC and/or poor public education on appropriate drug usage. A study in Central China showed that 77% of participants agreed that stewardship programs improve patient care and should be implemented at the community pharmacy level27.
According to some pharmacists, AMR may be impacted by local socioeconomic issues, drug resistance to the preferred chemotherapeutic agents, a lack of consultation time and a lack of national recommendations or guidelines28. Although this study did not query pharmacists on these particular points, the conditions of both Ghana and Lebanon are parallel to one another about economic stance. Therefore, these factors could be influencing the propagation of AMR. Similarly, Physicians in Saudi Arabia identified that inadequate prescriptions, self-medication and non-compliance of patients are the most important factors contributing to the development of bacterial resistance29. The same physicians blamed pharmacists for contributing mostly to the development of AMR and stated that they feel pressurized if patients expect an antibiotic prescription. The findings of this study show that 72.5% (n = 37) of physicians are asked by patients for a prescription for antibiotics. However, the study did not assess the physicians' personal or emotional opinions regarding this request and the perceived bearing it has on AMR.
The majority of the physicians in this study knew about the nonclinical/environmental routes for the spread of AMR genes while only 36.9% of physicians in Pakistan knew about the same possibility30. This might be an indication that physician education on AMR is better in Ghana than it is in some parts of the world. On the other hand, a competing study also conducted in a Ghanaian Tertiary Hospital showed that only 30.1% of physicians felt AMR was a global problem31. However, this study showed that 74.5% (n = 38) of physicians felt AMR was a problem they faced daily. This might be a definite indication that rates of AMR have risen in the last two years or conversely, physician education has improved. The AMR knowledge base of health professionals is sufficient to support any AMR stewardship program that is carried out to foster behavioral change. However, for a paradigm shift in attitude and behavior towards controlled antibiotic use, collective efforts from all facets of the community need to be harnessed.
CONCLUSION
These findings provide a thorough representation of AMR by three key players and captured views from respondents across all but two regions of Ghana. The continuous dependence on antibiotics for various curative purposes is highlighted. No adherence to the use of prescriptions for antibiotics cuts across both the educated and uneducated populace of Ghana. This study portrays a clear pathway of hitherto hypothetical areas such as the advertent use of antibiotics to treat extended colds, coughs and soared throats, hoarding for emergency self -administration then final disposal into waste bins. There is virtually no knowledge of appropriate modes of antibiotic disposal, a grey area for further research.
RECOMMENDATIONS
Per the alarming findings of this tri-group study, the authors make the following recommendations:
| • | Antibiotics should always be dispensed based on strict prescription | |
| • | Expired and leftover antibiotics should be disposed-off only after being secured in a zip-lock or sealable plastic bag | |
| • | The regulatory body for pharmacies should incorporate “take-back” programs to appropriately dispose-off drugs | |
| • | The Ministry of Health should establish a vigorous surveillance system where healthcare professionals can be informed about resistance patterns digitally | |
| • | The Ministry of Health should encourage effective communication forums for health professionals to streamline the process of testing, diagnosing and treating infectious diseases appropriately | |
| • | The Ministry of Health should organize public health talks addressing antibiotic use nationwide | |
| • | The professional regulatory bodies for pharmacists and physicians should organize mandatory CPD and stewardship programs on the subject of AMR | |
| • | It is recommended that a future study should assess the personal opinion of clinicians and pharmacists regarding patient requests for specific medications |
ACKNOWLEDGEMENT
The authors of this study are grateful to Dr. Jonas Danquah, Dr. Eric Nyarko, Ms. Ifeoma Chudi-Oji Onyedika and Ms. Ahlam Tunteiya Saani for their numerous support in executing this study.
SIGNIFICANCE STATEMENT
There have not been any local studies that collectively assess the patient, physician and pharmacist knowledge base and attitudes toward antibacterial chemotherapy in Ghana. Through monitoring upgrades and educational activities aimed at rationalizing antibiotic prescriptions, disposal procedures and consumption patterns to prevent AMR, it is possible to achieve important strategic goals including raising knowledge and understanding of AMR. Thus, this study becomes necessary to evaluate the knowledge and gauge the practices of the aforementioned primary stakeholders in the battle against AMR. This article would serve as a working document for the AMR platform in Ghana, as well as help, meet key targets of the National AMR action plan.
REFERENCES
- Aminov, R.I., 2010. A brief history of the antibiotic era: Lessons learned and challenges for the future. Front. Microbiol., 1.
- Yevutsey, S.K., K.O. Buabeng, M. Aikins, B.P. Anto, R.B. Biritwum, N. Frimodt-Møller and M. Gyansa-Lutterodt, 2017. Situational analysis of antibiotic use and resistance in Ghana: Policy and regulation. BMC Public Health, 17: 896.
- Lomazzi, M., M. Moore, A. Johnson, M. Balasegaram and B. Borisch, 2019. Antimicrobial resistance-moving forward? BMC Public Health, 19: 858.
- Bush, K., P. Courvalin, G. Dantas, J. Davies and B. Eisenstein et al., 2011. Tackling antibiotic resistance. Nat. Rev. Microbiol., 9: 894-896.
- Founou, R.C., L.L. Founou and S.Y. Essack, 2017. Clinical and economic impact of antibiotic resistance in developing countries: A systematic review and meta-analysis. PLoS ONE, 12: 0189621.
- Wernli, D., P.S. Jørgensen, S. Harbarth, S.P. Carroll and R. Laxminarayan et al., 2017. Antimicrobial resistance: The complex challenge of measurement to inform policy and the public. PLoS Med., 14: 1002378.
- Medina, E. and D.H. Pieper, 2016. Tackling Threats and Future Problems of Multidrug-Resistant Bacteria. In: How to Overcome the Antibiotic Crisis: Facts, Challenges, Technologies and Future Perspectives, Stadler, M. and P. Dersch (Eds.), Springer International Publishing, Cham, Switzerland, ISBN: 978-3-319-49282-7, pp: 3-33.
- Ahmed, S.A., E. Barış, D.S. Go, H. Lofgren, I. Osorio-Rodarte and K. Thierfelder, 2018. Assessing the global poverty effects of antimicrobial resistance. World Dev., 111: 148-160.
- de Kraker, M.E.A., A.J. Stewardson and S. Harbarth, 2016. Will 10 million people die a year due to antimicrobial resistance by 2050? PLoS Med., 13.
- WHO, 2015. Global Action Plan on Antimicrobial Resistance. WHO Library Cataloguing-in-Publication Data, Geneva, Switzerland, ISBN: 9789241509763, Pages: 45.
- Pires, D., M.E.A. de Kraker, E. Tartari, M. Abbas and D. Pittet, 2017. ‘Fight antibiotic resistance-it’s in your hands’: Call from the World Health Organization for 5th May 2017. Clin. Infect. Dis., 64: 1780-1783.
- Ashraf, M., Behar-E-Mustafa, Shahid-Ur-Rehman, M.K. Bashir and M.A. Ashraf, 2019. Emergence of Antimicrobial Resistance, Causes, Molecular Mechanisms, and Prevention Strategies: A Bovine Perspective. In: Bovine Science-A Key to Sustainable Development, Sadashiv, S.O. and S. Patil (Eds.), IntechOpen, London, UK, ISBN: 978-1-78985-606-4, pp: 45-64.
- Ayukekbong, J.A., M. Ntemgwa and A.N. Atabe, 2017. The threat of antimicrobial resistance in developing countries: Causes and control strategies. Antimicrob. Resist. Infect. Control, 6: 47.
- Obeng-Nkrumah, N., K. Twum-Danso, K.A. Krogfelt and M.J. Newman, 2013. High levels of extended-spectrum beta-lactamases in a major teaching hospital in Ghana: The need for regular monitoring and evaluation of antibiotic resistance. Am. J. Trop. Med. Hyg., 89: 960-964.
- Forson, O.A., E. Ayanka, M. Olu-Taiwo, P.J. Pappoe-Ashong and P.F. Ayeh-Kumi, 2017. Bacterial infections in burn wound patients at a tertiary teaching hospital in Accra, Ghana. Ann. Burns Fire Disasters, 30: 116-120.
- Dayie, N.T.K.D., R.E. Arhin, M.J. Newman, A. Dalsgaard, M. Bisgaard, N. Frimodt-Møller and H.C. Slotved, 2013. Penicillin resistance and serotype distribution of Streptococcus pneumoniaein Ghanaian children less than six years of age. BMC Infect. Dis., 13: 490.
- Duplessis, C., N. Puplampu, E. Nyarko, J. Carroll and H. Dela et al., 2015. Gonorrhea surveillance in Ghana, Africa. Mil. Med., 180: 17-22.
- Ocan, M., E.A. Obuku, F. Bwanga, D. Akena, S. Richard, J. Ogwal-Okeng and C. Obua, 2015. Household antimicrobial self-medication: A systematic review and meta-analysis of the burden, risk factors and outcomes in developing countries. BMC Public Health, 15: 742.
- Borquaye, L.S., E. Ekuadzi, G. Darko, H.S. Ahor and S.T. Nsiah et al., 2019. Occurrence of antibiotics and antibiotic-resistant bacteria in landfill sites in Kumasi, Ghana. J. Chem., 2019: 6934507.
- World Medical Association, 2013. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Med. Assoc., 310: 2191-2194.
- Kaba, A.J., 2020. Explaining Africa’s rapid population growth, 1950 to 2020: Trends, factors, implications, and recommendations. Sociol. Mind, 10: 226-268.
- Tavakol, M. and R. Dennick, 2011. Making sense of Cronbach's alpha. Intl. J. Med. Educ., 2: 53-55.
- Labi, A.K., N. Obeng-Nkrumah, E. Owusu, S. Bjerrum and A. Bediako-Bowan et al., 2019. Multi-centre point-prevalence survey of hospital-acquired infections in Ghana. J. Hosp. Infect., 101: 60-68.
- Al-Yasseri, B.J.H. and N.A. Hussain, 2019. Public knowledge and attitudes towards antibiotics use and resistance in Baghdad, Iraq: A survey conducted in outpatient department of university teaching hospital. Open Public Health J., 12: 567-574.
- Atif, M., S. Asghar, I. Mushtaq, I. Malik, A. Amin, Z.U.D. Babar and S. Scahill, 2019. What drives inappropriate use of antibiotics? A mixed methods study from Bahawalpur, Pakistan. Infect. Drug Resist., 12: 687-699.
- Abujheisha, K.Y., R. Al-Shdefat, N. Ahmed and M.I. Fouda, 2017. Public knowledge and behaviours regarding antibiotics use: A survey among the general public. Int. J. Med. Res. Health Sci., 6: 82-88.
- Hayat, K., P. Li, M. Rosenthal, S. Ji and Y. Fang, 2019. Community pharmacists' knowledge about antibiotics and their perceptions of and participation in community-based antimicrobial stewardship programmes: A cross-sectional survey from central China. Lancet, 394: 32404.
- Zahreddine, L., S. Hallit, S. Shakaroun, A. Al-Hajje, S. Awada and N. Lahoud, 2018. Knowledge of pharmacists and parents towards antibiotic use in pediatrics: A cross-sectional study in Lebanon. Pharm. Pract., 16: 1194.
- Al-Homaidan, H.T. and I.E. Barrimah, 2018. Physicians’ knowledge, expectations, and practice regarding antibiotic use in primary health care. Int. J. Health Sci., 12: 18-24.
- Waseem, H., J. Ali, F. Sarwar, A. Khan and H. Saleem Ur Rehman et al., 2019. Assessment of knowledge and attitude trends towards antimicrobial resistance (AMR) among the community members, pharmacists/pharmacy owners and physicians in district Sialkot, Pakistan. Antimicrob. Resist. Infect. Control, 8: 67.
- Labi, A.K., N. Obeng-Nkrumah, S. Bjerrum, N.A.A. Aryee, Y.A. Ofori-Adjei, A.E. Yawson and M.J. Newman, 2018. Physicians’ knowledge, attitudes, and perceptions concerning antibiotic resistance: A survey in a Ghanaian Tertiary Care Hospital. BMC Health Serv. Res., 18: 126.
How to Cite this paper?
APA-7 Style
Emmanuel,
O.U., Waqas,
F.B., Appiah,
C.A., Mahmoud,
F.C., Nattah,
E.M., Banu,
R.A., Banini,
A.E. (2023). Assessing the Knowledge, Practices and Attitude of Pharmacists, Prescribers and the Community Toward Antimicrobial Resistance in Ghana. Pharmacologia, 14(1), 61-71. https://doi.org/10.17311/pharma.2023.61.71
ACS Style
Emmanuel,
O.U.; Waqas,
F.B.; Appiah,
C.A.; Mahmoud,
F.C.; Nattah,
E.M.; Banu,
R.A.; Banini,
A.E. Assessing the Knowledge, Practices and Attitude of Pharmacists, Prescribers and the Community Toward Antimicrobial Resistance in Ghana. Pharmacologia 2023, 14, 61-71. https://doi.org/10.17311/pharma.2023.61.71
AMA Style
Emmanuel
OU, Waqas
FB, Appiah
CA, Mahmoud
FC, Nattah
EM, Banu
RA, Banini
AE. Assessing the Knowledge, Practices and Attitude of Pharmacists, Prescribers and the Community Toward Antimicrobial Resistance in Ghana. Pharmacologia. 2023; 14(1): 61-71. https://doi.org/10.17311/pharma.2023.61.71
Chicago/Turabian Style
Emmanuel, Osisiogu, Udochukwu, Fahad Bin Waqas, Calebina Ayeyi Appiah, Fareeda Ceeta Mahmoud, Emmanuel Mawuli Nattah, Regina Ama Banu, and Amanda Eyram Banini.
2023. "Assessing the Knowledge, Practices and Attitude of Pharmacists, Prescribers and the Community Toward Antimicrobial Resistance in Ghana" Pharmacologia 14, no. 1: 61-71. https://doi.org/10.17311/pharma.2023.61.71

This work is licensed under a Creative Commons Attribution 4.0 International License.